Novel Measurement for Performance Improvement Challenge
Medupi Rapid TB Diagnosis Tool
What is the name of your solution?
Medupi Rapid TB Diagnosis Tool
Provide a one-line summary of your solution.
The Medupi is an optical Tuberculosis (TB) testing device which provides low-resource primary health care workers with an accurate screening tool
What specific problem are you solving?
Tuberculosis (TB) is the world’s second leading cause of death from a single infectious agent, after COVID-19. Although TB is a worldwide scourge, more than 86% of the world’s TB burden comes from 30 high burden countries, of which 22 of them are low-and-middle income, which makes TB a disease of poverty. Our field work in India and South Africa which, together, make up 29.3% of the global burden, as well as in Brazil, has shown us the need for primary health care to have better, more affordable, screening tools in order to improve their overall TB service delivery.
According to the World Health Organization (WHO), Primary Health Care providers (PHCs) play a critical role in controlling TB through early detection of the disease and expedient referrals for treatment. However, in environments such as remote villages, refugee settlements, suburban townships, and urban slums, primary health care providers do not have acceptable (according to WHO’s standards, see below) to quality diagnostic tools that can give them a complete and accurate picture of the TB spread in their community in order to precisely assess the burden of the disease.
Without effective monitoring tools to estimate community spread, frontline health workers in resource poor environments have little means to understand what efforts to fight TB are working well and where further improvements are needed. There are simply too many TB cases going undetected to allow for the proper marshaling of resources required for elimination of TB, making the WHO’s End TB Strategy, which aims to eliminate deaths from the disease by 2035, difficult to achieve.
An illustrative example would be the results of the Ghanian national TB prevalence survey in 2013 which showed much higher than expected levels of TB among those tested—only 5% had previously been diagnosed with TB and were on treatment. Despite the countries’ standard operating procedure which stressed that all patients with TB symptoms be immediately screened and started on care, frontline health workers were presented with numerous barriers (lack of access to hospitals, lack of access to technology, isolation of facilities) to prevent this from taking place—and TB spread unseen through the population.
From our field experience, we can confirm that these barriers are not unique to one country, they are endemic in low income countries, in locations removed from accessing large and well funded hospitals. We, and our partners, have identified lack of access to effective and affordable tests as a key barrier that prevents PHC systems from fulfilling their key role in TB prevention in these environments.
To define what is an acceptable testing standard, we use the WHO’s ASSURED guidelines (affordable, sensitive, specific, user-friendly, rapid, equipment-free, delivered), which refer to standards for ideal tests for the developing world. Currently, very few tests for TB meet these standards that are accessible for low resource health workers.
The most widely used test for diagnosing TB (with more than 77.6 million tests performed each year) is Sputum Smear Microscopy (SSM) which has a sensitivity of under 50%, making it the lowest performing testing system among its peers. However, due to its low cost of about $1 per test, this is the most widely used test worldwide, and predominant in low income settings like the ones we studied in India, South Africa, and Brazil. A test with sensitivity this low cannot provide PHCs with the high quality population level data needed to tailor and improve their services to the level of TB circulating in their community.
A better option is a Nucleic Acid Amplification Test (NAAT) but, despite a WHO recommendation, the uptake and accessibility of these tests has been low. This is because they require specialized machines ($17k) and assays ($15/test), and require infrastructure such as reliable electricity, air conditioning, and a constant water supply, things that are simply not available at low resource primary health centers.
There is an urgent need for tests that are cheap enough to enable governments to actively over-test in communities. Tests which are fast enough (returns results in minutes, not hours or days) for patients presenting at PHC clinics to get initiated on treatment at an early stage, which are portable enough to be placed at every point in the healthcare system, and can be brought door-to-door, and easy-to-use enough to be administered by minimally trained health workers, such as India’s Community Care Workers (CCWs) who routinely cover a hundred people each day.
A device in the hands of health workers like CCWs will enable TB fighting programs to move at the pace of the disease and its transmission. It will enable real-time surveillance, surging of resources, localized quarantines, and care in communities which are often left out of the system. These kinds of TB tests could realistically move developing countries further toward achieving Sustainable Development Goal 3.3: ending the TB epidemic globally.
A multifaceted approach is required to eradicate TB, because testing alone will not address all the complexities of the disease and its combat. The world will need improved anti-TB drugs, treatment of the pool of latent TB infected people, the development of a better TB vaccine, and non-health interventions are some of the critical activities required to win the fight against TB. However, testing enables the entire public health infrastructure to work—without quality testing in abundance, the public health system is flying blind.
What is your solution?
Medupi, in the Sepedi language means gentle rain. This kind of rain is considered a blessing; a pleasant rain that soaks parched land, yielding a plentiful harvest. This pleasant rain is representative of what we envision health equity to be. As rain falls on everyone equally, we want to make healthcare accessible to everyone, regardless of class, wealth, race, or religious beliefs.
To move toward this goal, we piloted the Medupi Rapid Tuberculosis Diagnostic Tool with a goal to put a breakthrough TB test in the hands of primary health care workers in developing countries by 2023. The innovative Medupi system can provide industry leading accuracy and specificity at an affordable cost, and without needing extensive resources. The Medupi’s test sensitivity reaches 94% and its specificity reaches 90%. This rivals the much higher cost NAAT tests described in the previous section, without the need for the expensive and cumbersome machines. The cost is 2.00 USD per test, with a full setup costing a health center only 500 USD. Each test procedure takes 40 minutes, and a primary health worker can see results in minutes.
The Medupi is simple and easy to use, no matter what the skill level of the health care provider using the device, and is designed to be automated and minimize user error. The system is broken down into two pieces, which work together to deliver quick and accurate results.
The first piece is a cartridge, known as the MagnaSlide, which looks like a microscope slide but is made of polystyrene. It works like this: a patient presents a sputum sample in a cup, and a health worker extracts the sample from the cup and places it in the cartridge, which contains a polymer based microfluidic mechanism—a small channel with one side coated with a ‘sticky’ polymer. As the sample flows through the channel, the TB causing bacteria ‘sticks’ to the polymer and concentrates the sample in a small spot . When the sample is intensified like this it markedly increases the sensitivity and because the polymer concentrates the sample in one area it greatly reduces user error in sampling the wrong area.
In our trials, the cartridge increases the sensitivity of the test from the 50% found in standard SSM to over 90%, similar to NAAT tests, and reduces the limit of detection which will allow for samples with low bacterial loads to still show positive, making the device exceptionally useful is high HIV prevalence locations (people co-infected with TB and HIV often show very low bacterial loads).
The second piece of the Medupi is a portable (briefcase sized) optical reader system. Once the health worker inserts the cartridge in the reader, the reader utilizes the refraction of a light source (laser) that shines on the sample. These refractions are read by a digital signal processor within the reader, which generates a unique signature.
The algorithm within the reader then cross-references this signature against a library and determines what the specimen likely is. Then with no further help from the health care worker, the reader can identify the unique signatures of TB mycobacteria and produce a positive or negative result within minutes.
The reader also works on standard SSM slides, giving quick readouts, but with less sensitivity than with a MagnaSlide cartridge.
<insert image here>

While the Medupi represents a breakthrough for TB testing, there is also the potential to expand the system to test for other diseases, as the library of signatures is open ended. With an expanding library of signatures, we envision that Medupi could eventually become a system to deliver last mile diagnostics, not just for TB but for other high priority diseases in the future.
Who does your solution serve, and in what ways will the solution impact their lives?
We conducted field testing in India, South Africa, and Brazil, countries that are middle income and have public health systems of varying quality and locations with uneven prevalence of TB. This, we feel, helped us get a varied sample of how the Medupi system might work in different developing contexts—no one country is the same and contexts vary inside countries. What we have seen in our field work is that providing primary health care systems with an accurate data collection device will have a positive effect not just in empowering health care workers, but also in dramatically improving lives of the patients, and improving conditions in their communities.
From the perspective of health workers, the Medupi will greatly increase their ability to be more agile and effective in the fight against TB. When these workers have access to a test they can afford, that provides excellent quality results, and that is portable, they can test widely throughout the communities in which they work. In other words, the Medupi provides primary health care workers with actionable and accessible data insights of high quality that can be used not just to help patients get accurate diagnosis, but to get a better and more complete picture of TB prevalence in the community, so that limited resources can be better targeted to where they are needed most.
From the perspective of patients, Medupi offers them the chance at better access to the kind of healthcare data that they need to stop the ongoing transmission of TB. When patients have access to a fast and high accuracy test (for example at their homes with door-to-door testing, or when presenting at a primary health center for something else) they can receive a positive diagnosis for their TB and receive treatment before their infection worsens and they have transmitted the infection to those around them.
When getting a test means missing work and a chance to provide for their families, people will often instead neglect their symptoms or opt to treat themselves. They may then present at village centers/subcenters where they can be misdiagnosed. They may need to be referred to a hospital further away, resulting in more spread and more opportunity to abandon the whole process as work hours are compromised. They may also work while sick, with their condition going from bad to worse, with their ability to work well suffering. Currently, it can be up to 4 months from infection with TB to when an individual begins treatment.
According to the National Strategic Plan To End TB in India 2020-25, a 25% increase in active TB case finding by 2025 will decrease the TB incidence rate to 170 cases per 100 000 population. While, a 30%, 70%, or 90% increase in active TB case finding will result in a TB incidence rate of 148, 120, 44 cases per 100 000 population respectively.
For example, Rajasthan (where we have existing partnerships) has an estimated population of 81.2 million people and accounts for ~7% of the total TB burden in India. Currently, 89% of bacteriologically confirmed TB cases are performed using SSM, X-rays, and TB culture. With our technology being used to replace only 30% of the tests performed at PHCs, we could correctly diagnose an estimated 44, 954 TB patients in our first year of operation alone.
While we see Medupi primarily as a testing and data collection device that will improve TB monitoring and efforts for eradication led by primary health workers, we also recognize that Medupi could serve a role for marginalized populations in high income countries as well. For example, people experiencing homelessness (PEH) populations are not limited to developing countries, but are 4 times more likely than the overall population to have TB, including in developed countries.
There are also specific benefits of the high detection threshold of the Medupi for people living with HIV, including sex workers. In these situations, having a low level of detection is critical as TB bacterial load is generally very low, and they can go undetected by less accurate tests. These will be a specific target of our program when we follow our expansion plan from India to South Africa, where there is the world’s highest prevalence of HIV and AIDS.
How are you and your team well-positioned to deliver this solution?
Our core team at Drizzle Health is composed of Bonolo Mathekga and Digvijay Singh, born and raised in South Africa, and India respectively, where we have been witness to the effects of TB in our communities and seen the lack of primary care’s ability to control the problem with the data collection tools they have. Trying to provide better quality data, so that the existing heroes working on the front lines in countries like this can improve the delivery of something as important as public health has been the primary force driving our careers.
During our field research, both of us had extensive on the ground experiences working with Community Care Workers (CCWs) South Africa and India, going door-to-door in underserved areas providing TB services to their communities. Collectively, we have spent over 200 hours conducting stakeholder interviews with CCWs, community leaders, government officials, doctors, nurses, TB patients and their families, growing to understand the deep pain that this disease causes in a community, even as other diseases get the spotlight.
Bonolo went to the University of Witwatersrand in South Africa where she was awarded her bachelors in Information Engineering, and Biomedical Engineering while Digvijay studied Materials Science at the Indian Institute of Technology, Varanasi and worked in product design and ethnographic research for a few years.
When we were accepted to the Johns Hopkins Center for Bioengineering Innovation and Design for our masters, we were lucky enough to meet and eventually, with the guidance of mentors and other supporters, form the ideas that would eventually become our work today.
We can’t say enough about our mentors from Johns Hopkins University, who have been so supportive of this work and believe in the great potential to advance public health. We count among our believers and supporters those with extensive backgrounds in global health and infectious disease research, cutting-edge nanomaterials research as well as TB mycobacteria and epidemiology. Others are experienced in production, TB testing in primary and tertiary clinics, treatment of TB in communities, regulatory and state health machinery.
Throughout our design process, we have held numerous design sprints, ideation sessions and co-creation sessions with different stakeholders involved in the TB care pathway, right from CCWs to epidemiologists. We are also constantly engaging with our partners in India, South Africa, and the US, to get feedback on our design process. We're currently working towards hosting a virtual listening session with CCWs, TB patients, and researchers in South Africa to learn how reimbursement for CCWs works, as well as how the on-going Covid-19 pandemic is affecting active TB case finding at a community level.
Moving forward, we need even more support to sustain and grow our innovations. While we are blessed with strong support from academics and doctors, we need further support in other types of expertise—grant writers/global funding experts, production engineering experts, key opinion leaders in various communities, fundraising experts, specific target populations, etc. We anticipate that our team composition will evolve over time to reflect our learnings and engagement with target populations as well as our requirements for development and implementation; but this is a process we hope to accelerate through our involvement with the MIT Solve community.
Which dimension of the Challenge does your solution most closely address?
Where our solution team is headquartered or located:
Baltimore, MD, USAOur solution's stage of development:
PrototypeHow many people does your solution currently serve?
We are currently in the testing phase. In our field tests, we worked with a sample population of 100 patients in India and 33 previous patients in Uganda. We anticipate that we will be able to submit data to our partners by November 2022. We then plan to begin sales and serving by early 2023 through the use of the MagnaSlide in microscopy based testing. We anticipate that our data for the complete Medupi system will be finalized and we will begin sales and serving by the end of 2023.
Why are you applying to Solve?
Aside from the incredible prestige and honor that would come with being awarded as a Challenge winner by an institute like MIT, we are looking to get specific things from the experience of being part of the solver community. Our goals have always been to grow our team, to expand our research partnerships, and increase the breadth and depths of our connections in the world—we do not believe that we can make the changes we need to see in this world we live in while siloed in our company.
As we complete our transition from research, to design, to going to market, we're looking for mentorship, partnerships, funding and hiring for our company. We feel that being a solver could open the doors to us for these specific kinds of support
1. Partners for field trials: We’ve currently been depending on a single field partner, which has led to delays and has limited the width of our study. We're looking to engage with partners who can use our devices in their projects and settings and not only help create field data, but also iterative design changes based on specific population feedback.
2. Partners for research: While we are excited to say we have new research partnerships with the Sexually Transmitted Diseases group at Johns Hopkins, we are also looking for partners working in research settings outside of the University. The Medupi, as mentioned above, has potential for the reader to expand the ‘signatures’ which it recognizes in the reader. We want to work with partners who can help us broaden the library and see if we can’t put this technology to use for rapid testing of other infectious agents.
3. Fundraising partnerships: We have been extremely happy with the support we have received so far from the academic world, but we want to move beyond that and find other people excited enough about what we are doing to back up with funding. Other than keeping the lights on, we're looking to reimburse and pay for larger field studies beyond our upcoming one.
4. Personnel: We are a strong team, but we are a small team, and we know that we can’t do what we need to do alone. We need to surround ourselves with a supportive community who is as passionate as we are about ending TB. We're looking to hire great people—engineers in materials, optics, electronics and production/manufacturing to support engineering requirements of the project, and a full time fundraiser.
5. Practical mentorship: Navigating fundraising, approvals through governments and official bodies, and expanding our network to include more buy-in from the customer.
Moreover, being a part of an environment that fosters creativity and growth, is invaluable to us as individuals, and even more so as a team.
Who is the Team Lead for your solution?
Bonolo Mathekga
What makes your solution innovative?
As we showed with the example from the Ghanaian TB survey, there is a great deal of silent TB spread in low-income countries, especially those with a high detected burden of the disease. As TB can stay latent for a long time, and a patient can then transmit rapidly when symptomatic, it can be very difficult to muster a plan to battle the disease. Imagine being on a battlefield when you are acting on information that is days, weeks, even months old. That would not be a battle that could be won.
Medupi is unique in that it is a proactive test that can move along at the speed of TB transmission at a community level instead of encumbering health workers with ‘best they can do’ testing that provides poor quality results too late to make a difference at a community level. Medupi, on the other hand, allows CCWs and health practitioners to do active case finding door-to-door, area-to-area, and conduct effective contact tracing in their communities—something that research done in Thailand, republished by the WHO, describes as an imperative intervention.
As patients who are tested with the Medupi get their results in their first contact with a health worker to be tested, they can initiate treatment right there and then. This extremely fast turnaround can help governments sweep entire communities very quickly, put local micro-quarantines, and provide support resources with precision. This can only be enabled if testing is low cost enough, returns results fast enough, can be mobile and used with minimal training.

Our approach and device design paves way for the agility and interoperability needed to stop these vicious hidden cycles of community spread that often have devastating effects on the health, finances and humanity of people and families.
We believe that this model will ultimately be able to support other community based diseases, using research and data from other groups and organizations in the field - In the long run, we envision strong local ecosystems run for the community and by the community.
What are your impact goals for the next year and the next five years, and how will you achieve them?
We are seeking to achieve the following metrics in our first 2 years.
Short-term (first 2 years, since we need to await approval post testing) - (Through Cartridge sales only)
Increase the number of bacteriologically confirmed TB cases by 20% in Chennai, India.
Increase TB notification rates by 50>#/p###
Patients get correctly diagnosed the first time at least 90% of the time
Ease of accessibility encourages more people to get tested
Reunite patients with their test results on the same day
Initiate patients on TB treatment within 24 hours from diagnosis
Long-term (2-5 years) (Use of the complete Medupi system)
All and any presumptive TB patients, when accessing public healthcare, will get correctly diagnosed, which will create a positive impression of the system and process
There will be a 20% decrease in TB incidence rates and deaths
Increased population covered in active tracing efforts by 50>#/p###
A 25% reduction in number of hidden TB patients
Doctors’ distrust on the utility of point of care tests for TB is reduced
Increases quality of life amongst afflicted population
Reduce TB stigma due to faster relief from signs and symptoms
Reduced incidence rate of multi/extreme-drug resistant TB (due to improved monitoring of active TB cases)
Establish TB outbreak surveillance in under-served areas
We will achieve our impact goals by using our products to test presumptive TB patients at point of care settings. We will work alongside CCWs, and lab technicians to conduct TB testing and report the results to both the patients and the national TB registry in a timely manner.

We currently have partners in place to produce our beta prototypes of our cartridges upon approval at scale (in the thousands). As we finish our detailed engineering phase for our cartridges, we will be working with our existing partners, also looking for new partners, to scale our production to the hundreds of thousands.
We are looking for partners and organizations that have gone through the process of mass manufacturing complex electronic products - While we currently have a bill of materials based on high level designs from vendors, we're looking for support in planning and manufacturing for our Medupi reader while it undergoes a detailed engineering phase.
As shown in the timeline above, we will begin with small pilots of the cartridge in 2 states (Uttar Pradesh and Rajasthan) - While we plan to work through the state health departments in this location, we are also looking for partners already working with target populations in these states so can we can add the Medupi to their efforts.
We will then expand our program in the states over the next year. We will both work
1. with partners
and
2. directly with state health departments for roll-outs within state health infrastructure.
How are you measuring your progress toward your impact goals?
We are planning, over the first few of the Medupi rollout, to track the following indicators toward our goals.
Increase number of bacteriologically confirmed TB cases by 20% in Chennai, India
The Indian government requires the reporting of all detected TB cases. Since Medupi is already connected to a laptop, we can simply integrate data collection of the number of positive test results that were detected using Medupi. This data will be compared alongside the TB detection rates of previous years (before Medupi was introduced). We plan to track the performance of Medupi in Chennai for one year and achieve at least a 20% increase in the number of bacteriologically confirmed TB cases.
Patients get correctly diagnosed the first time at least 90% of the time
Since Medupi is a screening tool, patients that test positive using this device will be referred to a PHC to receive confirmatory tests, as well as initiation on anti-TB drugs. We are aiming to achieve concordance with the confirmatory test method in at least 90% of positive TB test cases within one year of monitoring the performance of Medupi in Chennai.
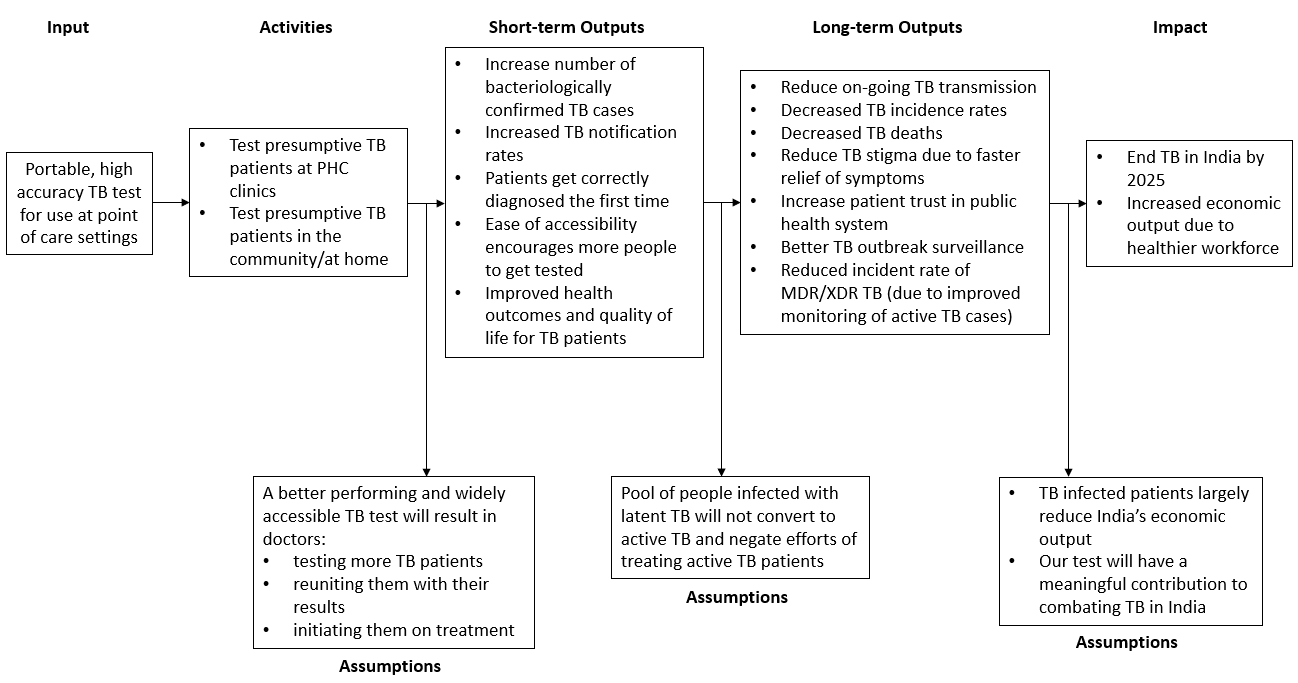
What is your theory of change?
The ultimate outcome for the Medupi is to contribute towards making India TB-free by 2025, in alignment with the Indian Government’s TB Free India Campaign.
We will build toward this ultimate outcome by achieving a series of intermediate outcomes:
1: Reduction of on-going TB Transmission in India
2: Decreased TB incidence rate in India
3: Decrease deaths from TB in India
4: Reduction of TB Stigma (less obvious symptoms)
5: Increased patient trust in primary health care
6: Improved TB Surveillance
7: Reduced incidence of MultiDrug Resistant (MDR) and Extensively Drug Resistant (XDR) TB in India
We will achieve these goals with the following outputs:
We will increase the number of bacteriologically confirmed TB cases by 20>#/p###
We will increase the TB notification rates by 50>#/p###
We will ensure patients get correctly diagnosed the first time at least 90% of the time
We will increase ease of accessibility encourages more people to get tested
We will ensure patients receive their test results on the same day
We will help Initiate patients on TB treatment within 24 hours from diagnosis
See our complete Theory of Change below
Describe the core technology that powers your solution.
The cartridge is powered by our polymer system that concentrates TB causing bacteria to one spot. The TB-capturing cationic polymer system, poly diallyldimethylammonium chloride (pDADMAC) has previously been shown to have a high affinity for mycobacterium [1-4]. The polymer system is used in a microfluidic chip optimized for increasing contact time of the bacteria with the polymer for a variety of input velocities. Non-provisional patent has been filed.
The reader makes use of a polarization imaging technique to probe the microstructural and optical information of TB bacterial colonies [5]. The system is composed of an optical light transmitter and receiver, which detect the presence of a unique TB signature on the cartridge. Optical signals are then processed and analyzed by comparing it to an existing library of bacterial signatures, thus leading to a positive or negative TB test result. Provisional patents have been filed.
[1] Albert H, Ademun PJ, Lukyamuzi G, et al. Feasibility of magnetic bead technology for concentration of mycobacteria in sputum prior to fluorescence microscopy. BMC infectious diseases
2011;11:125.
[2] Liu J, Sun ZQ, Pei H, et al. Increased case finding of tuberculosis from sputum and sputum deposits after magnetic bead concentration of mycobacteria. Journal of microbiological methods
2013;93:144-7.
[3] Wilson S, Lane A, Rosedale R, Stanley C. Concentration of Mycobacterium tuberculosis from sputum using ligand-coated magnetic beads. Int J Tuberc Lung Dis 2010;14:1164-8.
[4] Tadesse M, Aragaw D, Rigouts L, Abebe G. Increased detection of smear-negative pulmonary tuberculosis by GeneXpert MTB/RIF(R) assay after bleach concentration. International journal of mycobacteriology 2016;5:211-8.
[5] Badieyan, Saeedesadat, et al. "Detection and discrimination of bacterial colonies with Mueller matrix imaging." Scientific reports 8.1 (2018): 1-10.
Which of the following categories best describes your solution?
A new technology
Please select the technologies currently used in your solution:
Which of the UN Sustainable Development Goals does your solution address?
In which countries do you currently operate?
In which countries will you be operating within the next year?
Who collects the primary health care data for your solution?
Community Care Workers
CCWs are already tasked with conducting door to door visits to patients' homes, increasing community education on infectious and communicable diseases. In India, for example, the ASHA workers are employed by the Ministry of Health and Family Welfare (MoHFW) as a part of India's National Rural Health Mission (NRHM). CCWs typically collect data through notebooks (as witnessed during our ethnographic research in South Africa), or a small portable electronic device (i.e. tablet/smartphone).
What type of organization is your solution team?
For-profit, including B-Corp or similar models
How many people work on your solution team?
2 Full-time, 1 part-time, 3 advisors, 2 part-time interns, 6 contractors
How long have you been working on your solution?
3 years
What is your approach to incorporating diversity, equity, and inclusivity into your work?
As a team, we firmly believe in acknowledging our differences in race, color, sexual orientation, gender identity, religion, disability, age, genetic information, veteran status, ancestry, and national or ethnic origin. It is only by acknowledging what makes us different, that we are able to truly embrace and celebrate our diversity. These differences govern how we uniquely experience the world, and motivate our decisions on when and how we access healthcare, the type of diseases endemic in our communities, and the medications available to us.
Our goal is to fight TB and the destruction it is causing millions of lives around the globe each year. We understand that this is a fight where we need all the help we can get and need to rely on the best of each other.
The team's co-founders have differing backgrounds. Digvijay is an Indian national, hailing from the national capital region. Bonolo is a South African woman of color. Both are immigrants to the United States.
This spirit is reflected in our current team and extended team, and will guide us as we expand.
What is your business model?
Our primary business model is based on the Razor Blade business model: Charge per device and cartridge, with a recurring profit margin over cartridges.
We plan to sell each cartridge for $1-1.5 (NAAT based systems require cartridges costing around $15 each). Our proposed price point falls well within guidelines set by the Foundation for Innovative New Diagnostics (FIND) and the World Health Organization's (WHO) Target Product Profiles. At scale, the bill of materials for the cartridge falls at under $0.25.
We plan to sell each device for $1000-3000 (awaiting pricing interviews with stakeholders). At scale, the bill of materials for the optical reader falls at under $1000.
For the purposes of our 1-3 year plan, our customer is the Government(s) of India (states and ultimately center). The central government has declared that they'll make the country TB-Free by 2025 - There's political capital attached to the massive goal. This is an urgent problem for them. Diagnostics is a huge part of that problem. And there's a lot of initiatives and finances that have been set in motion to achieve that goal.

(Source: National Strategic Plan to End TB in India 2020; Scenario SDG denotes scenario for achieving TB free country)
The National Strategic Plan to End TB in India 2020 report shows that, according to the government's own estimations, India will need to conduct 6 times more tests and over 90% of the population will have to be screened in order to achieve the results needed.
Last year, 10 million tests were conducted in India. To do this number of tests, using NAAT, over 5 years would cost $750M. However, to continue to test at the rate India would need to in order to conduct 6 times this amount of tests, the cost would rise to a staggering $4.5B. In our initial target states of Rajasthan and Uttar Pradesh the expenditure on testing was $7.8M and $4.8M on diagnostics alone. To attain SDG scenarios, just these two states would need to spend $240M and $150M over 5 years. Such high numbers are unsustainable without foreign aid, which is rapidly shifting to other diseases such as Covid, and to other priorities such as the humanitarian crisis in Ukraine.
Using our device, India's 5 year cost would only be $300M. This results in massive savings with no loss in quality. With this kind of money freshly available, state governments could not only increase funding for treatment, but also:
1. Test all people presenting with symptoms
2. Test contacts of people presenting with symptoms (contact tracing)
3. Conduct door-to-door screening, impose 'mini-quarantines' based on instantaneous (not weeks old data) (active case finding)
4. Monitor treatment of patients initiated on treatment and track drug-resistant cases.
This can only be possible due to low device and per test costs, AND the almost immediate results.

This graph shows the impact of using Medupi on a large scale in our initial target states of Uttar Pradesh and Rajasthan, without increase in funding allocation for diagnostics in the states. This shows a direct impact for our customers (state governments) and beneficiaries (patients) sustainable over a long period of time.
Based on the current timeline projection, we're targeting sales of 1 Million cartridges by the end of 2024, and sales of 100 Medupi readers by the end of 2024. While we continue to cultivate contacts with state health officials, finding channels to purchase and approval departments (in India and outside India) is something we can use MIT SOLVE community's help with.
For scale, there were 8.2 million microscopy based tests and 2.3 million NAAT based tests done in India - This is the size of the current total addressable market which is slated to grow 5 times by the government's current estimation. We hope to start with pilots in 2 states, before expanding to other states and finally to the national TB program. The number of new patients in India was about 1.9 million in 2021. Worldwide, there were about 10 million patients.
Do you primarily provide products or services directly to individuals, to other organizations, or to the government?
Government (B2G)What is your plan for becoming financially sustainable?
As explained before, the overall long strategy is to start with the Indian market, and then expand to South Africa.

We're currently bootstrapping, as planned, to finish phase I (i.e. collect field efficacy data at YRG, Chennai). Once field efficacy data is in, we'll get back to various India based grant funding partners we've been in touch with. We also plan to hire a full-time "grants-person" to help us with actively pursuing grants as we transition towards Phase II activities. Towards our bootstrapping strategy, our company has been and continues to provide consulting services to the National Institutes of Health's (NIH) Rapid Acceleration of Diagnostics (RADx) initiative.
From a product perspective, the strategy is to pursue separate approval paths for the cartridge and the whole Medupi system. The cartridge is a relatively simpler and lower cost product that we already have a lot of buy in for. It also has a lower regulatory burden, as per the Central Drugs Standard Control Organization's (India's medical devices regulatory body) guidelines and has extreme utility for the equipment used by the Indian TB program now, and for the foreseeable future.
The Indian government, in 2021, released an essential equipment list enumerating equipment it seeks to procure for health centers at every level - this includes microscopy equipment for TB at various levels, indicating that apart from a strategy focused on NAAT, the government is actively procuring and putting infrastructure in place for microscopy.
Since the cartridge readily works with microscopy, and dramatically increases performance, we see it as a low barrier first product that will bring in revenue in the short term, while we work on the engineering, regulatory and production scale-up phases for the Medupi reader and No comments to show.
Solution Team
-
 BM
Bonolo Mathekga Miss, Drizzle Health, LLC
BM
Bonolo Mathekga Miss, Drizzle Health, LLC -
DS
to Top
Our Organization
Drizzle Health LLC